2021.06.03.19
Files > Volume 6 > Vol 6 No 3 2021
Role of Candida glabrata as nosocomial pathogen and its susceptibility to Fluconazole, Voriconazole, Caspofungin, Micafungin and Amphotericin B

Teeba Hashim Mohammed 1, Mohsen Hashim Risan 1, Mohammed Kadhom2, Emad Yousif3, *
Available from http://dx.doi.org/10.21931/RB/2021.06.03.19
ABSTRACT
Candida has different types that could cause bloodstream infections. A total number of 150 samples were collected from candidemia patients and examined. The Candida spp. Species isolated from blood samples were analysed. These were identified by culturing the species using different media, namely the chromogenic agar test. Then, the virulence factors of all samples were tested. The Candida glabrata isolates were tested with six commercial antifungal drugs. C. glabrata 67 (44.6%), C. albicans 34 (22.6%), C. krusei 18 (12%), C. tropicalis 17 (11.3%), and C. parasilosis 14 (9.3%). the production of phospholipase ranged between 0.63-0.99 mm. It was found that 96% of the species showed phospholipase activity in aerobic conditions. The protease activities of Candida spp. Isolates were experimentally tested by area of inhibition around the colonies, where 59.3% had the double (++) protease activity, 31.4% with (+) grade, and 9.3% had (–) grade or clear zone around the colony. The hemolytic capacity ranged from 0.69-0.89 in the optimum aerobic environments. Finally, 38.33% of the isolated Candida spp. were positive and 61.67% negative for biofilm formation. Out of the total positive Candida spp. for biofilm formation, 21.73% were strong biofilm producers, and 78.27% were weak. Minimum fungicidal concentration (MFC) of Fluconazole for C. glabrata isolates was not appropriate (NA) due to the occurrence of low inhibition tested for species. Micafungin exhibited the lowest fungicidal activity against C. glabrata ranging from 0.03 - 0.125, while Fluconazole showed the highest.
Keywords: Candidemia; chromogenic agar; Candida glabrata; Antifungal
INTRODUCTION
Candida is a significant genus of Ascomycete fungi, commonly called yeast, consisting of approximately 150 species, more than 20 of them of clinical importance1. Candida spp. became the fourth most public reason for bloodstream infections (BSI) more than two decades ago2,3. The highest occurrence rate was described in the USA4, where candidemia signifies an essential danger for hospital patients5. Hence, C. albicans and C. glabrata remain the primary cause of aggressive candidiasis, responsible for 50% of all cases followed by other species of Candida, such as C. tropicalis and C. parapsilosis6,7.
The effect of Candida species is presented by interrupting BSI incidents; their phospholipase and protease activity and the sensitivity towards the main antifungal agents were available 8. Described mortality data comprised the age, period of hospitalization, skin infection, severe renal failure, preservation of the dominant venous line, and mechanical ventilation9, 10. The germs become active at 37 °C, where protease and phospholipase are produced and facilitated adherence to the surfaces of host cell membranes; these were measured to be significant factors in starting the infection. Proteinase and phospholipase release can prime the membranes dysfunction or uniform rupture that assists the microbe to adhere to the host11. The communication in the pathogenesis of aggressive candidiasis, proliferation in fungal colonization is the best significant factor in the invasive candidiasis for pathogenesis. The density and colonized apparent area are responsible for the strength of the infection. Precise identification of Candida species helps control the hazards of candidemia infections and transmission from exogenous sources in certain patients12. Virulence factors are also associated to a great degree with the antifungal resistance shown by the microorganisms.
Furthermore, the capabilities of Candida species to produce drug-resistant virulence factors are significant in their development of human disease13. Recognition of Candida to the type's level is significant to improve the range of the antifungal agent to be prescribed. On the other hand, essential and developing resistance to azoles characterizes a significant trial for experimental, therapeutic, and prophylactic approaches. The range of candidemia has altered with the appearance of C.glabrata species, a strain with the hazard of increased transience and antifungal treatment of drug resistance, particularly in immunocompromised and very ill patients. The situation is very significant to recognize Candida to the type's level to improve the range of the antifungal agent 14.
MATERIALS AND METHODS
Collection of samples
Samples were collected from 150 patients with leukaemia and dialysis who were hospitalized at Madinat Al-tib hospital. The collection continued over four months, from September 2019 to January 2020. Processes of blood culturing and yeast segregation were conducted in the fungus laboratory at the College of Biotechnology/ Al-Nahrain University. The blood samples were inoculated on an SDA medium with chloramphenicol. All plates were incubated at 37°C±1 for 24, 48 hrs. Later, samples were examined and biochemical tests were performed to confirm the diagnosis of the species; the approval was obtained to take blood samples from the hospital administration and the discharged patients.
Isolation of Candida spp
Samples were inoculated on the appropriate culture medium containing sabouraud dextrose agar with chloramphenicol. All plates were incubated in aerobic conditions of 37 °C for 48 h15.
Identification of Candida spp. Isolates
First, single colonies were separated from the prime positive cultures; then, they were isolated according to published protocols16 that involved the following examination. All isolates were grown on sabouraud dextrose agar and incubated at 37 ºC for 48 hrs. Pure isolates of Candida colonies were examined to explore their form, size, color, and surface. Chromogenic agar plates were inoculated by streaking. Candida colonies using sterile loop then incubated at 37 Cº±1 for 48 hrs. The growth and color of colonies were observed.
The medium was prepared by dissolving 45.9 grams of the standard medium in one liter of purified water, mixed well, and melted by heating with repeated agitation. The mixture was boiled for 2 minutes until the complete dissolution and was not autoclaved17.
Virulence Factor Tests
The quick preliminary medical identification of Candida spp. usually depends on the detection of germ tubes from Candida cells, where their width or length is about three to four times the size of the cell. Candida spp. cells were added to 1000 μl of human serum with a sterilized loop, and incubated aerobically for three hours at 37 ºC. Then, cells were visualized under a microscope18.
The egg yolk agar technique is used to test the phospholipase activity19. The culture medium contained of 1 L of SDA comprising (1M NaCl, 0.005 M CaCl2, and 10% egg yolk). From prepared yeast suspension, 10 microliters were taken to one McFarland (3×108 CFU/ml) inoculated at 37 Cº for 48 hr. in the petri dish, 3 replicates per sample. After that, it was incubated at 37 °C for 3 days in aerobic conditions; the significance of phospholipase action was calculated with this formula: (Pz value= Colony diameter/ (Colony diameter + zone of precipitation)20. To test the proteinase activity, bovine-serum albumin agar was used. The prepared agar consisted of 0.1% KH2PO4, 0.05% MgSO4, 2% agar, and 1% bovine serum albumin at a final pH of 4.5. Similar inoculation aerobic conditions as above were applied for 48 h. The existence of the proteinase activity test was determined by observing a clear zone around the Candida spp. colonies21. Regarding the structural haemolytic action, SDA consisted of 7 ml human blood, 3g glucose, and 90 ml of sterile media was prepared using an autoclave with a final pH of 5.6 ± 0.2. 10 microliters were taken to one McFarland (3×108 CFU/ml) inoculated onto a dish; this was replicated 3 times per sample. Then, it was incubated at 37 °C for five days in aerobic conditions. After incubation, a clear/semi-clear zone around the yeast colony was detected as a positive haemolytic activity. The significance of hemolysis activity (Hz) was tested according to the equation: Hz rate = Colony diameter / (Colony diameter + Zone of precipitation) Agreeing to this scheme, activity kinds were recognized allowing to the Hz catalogue: Hz<0.69= very strong (++++), Hz = 0.70- 0.79= strong (+++) , Hz = 0.80- 0.89= slight (++), Hz = 0.90- 0.99=frail (+), and Hz =1 that is to say "Negative" results22. Biofilm production was tested using different recognition tests for Candida spp., which needs the use of a specifically prepared brain heart infusion broth (BHI), solid medium supplemented (agar) with glucose and Congo red indicator. The medium contained BHI (37 gm/L), agar no.1 (10 gm/L), glucose (80 gm/L), and Congo red stain (0.8 gm/L) as an indicator 23.
Determination of minimum inhibitory concentration (MIC) of several antifungals for Candida glabrata
The MIC of Fluconazole, Voriconazole, Caspofungin, Micafungin, Amphotericin B, and Flucytosine against Candida glabrata was determined broth microdilution method established on the Clinical and Laboratory Standards Institute (CLSI) natural resistance + base (bioMerieux, USA). Manufacturers' recommendations were strictly followed to obtain adequate measurements, which confirmed sterility and efficacy of the prepared media and used mixtures. Card type AST-YS07 of a barcode no. 287 (bioMerieuxm, USA) was used with an analysis time of 24 hours24.
Determination of MFC for Candida glabrata
For MFC determination, samples with different concentrations of MIC and C. glabrata were subcultured in Petri dishes containing SDA and incubated at 37 °C for 48 hours. The MFC is the minimum product concentration that stops apparent growth; it is the minor concentration capable of killing the yeast25.
RESULTS
Group’s classification
In this study, 150 samples were taken from three groups. The first group comprised 50 infected patients (women and men), as illustrated in Table 1; the second group comprised 50 patients of children with leukemia (Table 2); the third group comprised 50 patients with dialysis (women and men), as listed in Table 3. The first and third groups were divided into five categories, while the second group contained three subcategories. Generally, it was found that the total number of infected patients with Candida present in the bloodstream were isolated as follows: 67(44.6%) with C. glabrata, 34 (22.6%) with C. albicans, 18 (12%) with C. krusei, 17 (11.3%) with C. tropicalis, and 14 (9.3%) with C. parapsilosis

Table 1. Age group relationship with the number (and percentage) of infected patients with Candida spp from blood samples for adults (women and men).

Table 2. Age group relationship with the number (and percentage) of infected patients with Candida spp from blood samples for children.

Table 3. Age group relationship with the number (and percentage) of infected patients with Candida spp from blood samples of patients with dialysis for women and men.
Determination of Candida species by Chromogenic agar Medium
Candida spp was cultivated in a chromogenic agar medium plates and the characteristic dyed colonies were obtained after incubation; the medium supported the development of all isolates. C. albicans isolates produced green colonies when incubation for 48 h, while C. glabrata formed light pink smooth colonies and C. krusei colonies were pink; the distribution graduated from a light surrounding to a dark center. Also, C. tropicalis color was dark blue and C. parapsilosis formed pale colored colonies 26 as shown in Figure 1.

Figure 1. Observation of Candida spp. in Chromogenic agar media, (a) C. krusei, (b) C. albicans, (c) C. tropicalis, (d) C. glabrata, and (e) C. parapsilosis.
Determination of Virulence Factors for Candida Species
The development of germ tubes was achieved, as long tubes, within 2 hours, and positive results of Candida albicans isolates were observed, while no C. tropicalis production within that time was detected, as shown in Figure 2.

Figure 2. Germ tube of C. albicans growth on human serum at 37°C for 2hrs (40 X).
The germ tubes were grown in an incubator, and a particular diagnostic was used for distinguishing the C. albicans by separating it from other yeasts. Other species of yeasts, in general, did not produce germ tubes during this 2-hour incubation period. The Pz value varied between 0.63–0.99 mm when species were measured. It was found that 144 (96%) Candida spp. isolates expressed phospholipase activity in aerobic conditions, whereas the rest did not. Candida spp. possibly vary depending on the species and basis of isolates; Figure 3 shows the phospholipase activity of different Candida types on egg yolk agar medium.

Figure 3. Phospholipase activity of (a) C. krusei, (b) C. albicans, (c) C. tropicalis, (d) C. glabrata, and (e) C. parapsilosis) on egg yolk agar medium at 37 °C for (24-48) hrs.

Table 4. Phospholipase activity of Candida spp on egg yolk agar medium at 37 °C for (24-48) hrs.
The protease activities of Candida spp. isolates were tested for 3 days after an inoculation loop on bovine-serum albumin agar by the inhibition area around the colony. Eighty-nine (59.3%) isolates had the double (++) protease activity, while the grade (+) of protease activity was for forty-seven (30%) of isolates and fourteen (9.3%) had the grade (–) or clear zone around the colony as shown in Figure 4.

Figure 4. Protease activity from (a) C. krusei, (b) C. albicans, (c) C. tropicalis, (d) C. glabrata, and (e) C.parapsilosis on bovine-serum albumin agar at 37°C for (24-48) hrs.

Table 5. Protease activity from Candida spp on bovine-serum albumin agar at 37°C for (24-48) hrs.
Commonly, the hemolytic index is 0.69–0.89 in optimal aerobic environments. In this study, all experimental Candida spp isolations from blood samples had hemolysis activity when cultivated on SDA involving 7% human blood and 3% glucose.
Out of all Candida spp. isolates, the biofilms were 81(54.4%) negative, 28(18.6%) strong positive, and 41(27%) weak positive resulted from patients with leukemia and dialysis who are lying in hospital. The number of recovered Candida spp. from experimental samples was C. glabrata 34(49.2%), followed by C albicans (15.8%), C. krusei (12.5%), C.tropicalis (11.6%), and C. parapsilosis (10.9%). Among all Candida isolates, 46% were positive biofilm, and 54% cases were harmful biofilm. However, within the positive Candida biofilm, 21.73 % were strong biofilm producers, and 78.27% were weak; Figure 5 shows the biofilms.

Table 6. Biofilm formation results of 150 Candida isolated by Congo red agar
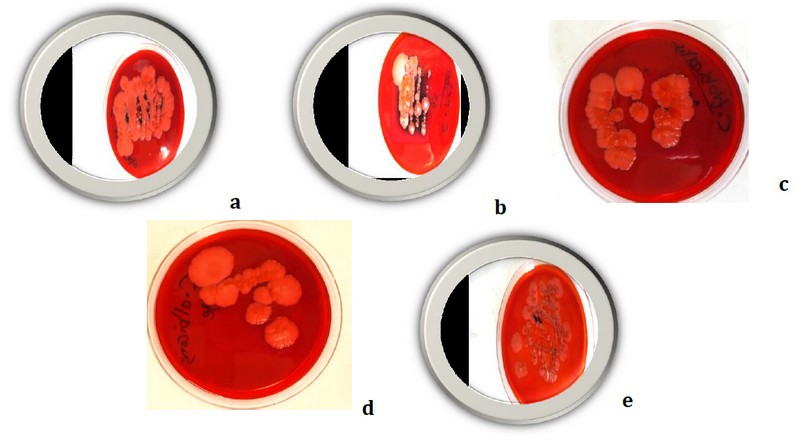
Figure 5. Biofilm formation resulted by (a) C. krusei, (b) C. albicans, (c) C. tropicalis, (d) C. glabrata and (e) C. parapsilosis on Congo red agar
Determination of MICs for Candida glabrata
The results of the susceptibility analysis of Candida glabrata isolates are summarized in Table 7. In all examinations, the minimum inhibitory concentrations (MICs) of the control C.glabrata isolated yeast were within the recognized limits (data are not shown). However, the CLSI's wild-brand MIC distributions were tested against six commercial antifungal drugs, namely: Fluconazole, Voriconazole, Caspofungin, Micafungin, Amphotericin B, and Flucytosine. The results showed that Fluconazole was the most active antifungal against Candida glabrata with different concentrations, whereas micafungin was the lowest antifungal resistance against Candida glabrata.

Table 7. Minimum Inhibitory Concentration (MIC) for C. glabrata isolates
The MFC ranges for the six drugs though significant change for the different organisms. Fluconazole, Voriconazole, and Flucytosine showed fungicidal activity against C. glabrata (MFC50s where appropriate ≥1 g/mL). MFCs of Fluconazole for this yeast was not appropriate (NA) due to the occurrence of small inhibitions tested number for species; table 8 illustrates this.

Table 8. Minimum Fungicidal Concentrations (MFC) for C. glabrata
DISCUSSION
Hospitalization (especially in cancer cases), location of central venous dialysis, and who preceding antimicrobial therapies control the number of candidemia infections. Candidemia in this concept was related to the prolonged stay (more than 15 days) of patients27. It is essential to mention that elder patients were more likely to receive insufficient antifungal therapy. Candidemia is connected with high mortality rates, increasing the hospitalization staying period, and raising therapeutic care28. The production test of the germ-tube has the benefit of being simple, effective, inexpensive, and fast to identify the Candida spp29. The chromogenic agar media are different; a selective medium was used to identify Candida spp fast. As a result, the capability to distinguish these species macroscopically was achieved 30.
The impact of the phospholipase enzyme was presented by digesting the cells' membrane of the host, producing cell lysis, and altering the external structures that increase adherence and result in infection. Therefore, phospholipase is possibly used as one of the limits to distinguish virulent hostile strains from non-hostile colonizers 20. Mohandas and Ballal, (2008)31 was referred that Candida spp. isolated from blood has more phospholipase activity. In two different studies from Turkey Candida isolates from blood culture, phospholipase activity resulted was (60.3% - 100%). The differences in results were retained because of distinctions in the sources of yeast isolates and the percentage of occurrence of isolates32.
The essential protease enzyme of Candida spp. evades the attack of host tissues. The majority of tested Candida spp. had a positive protease activity. These conclusions propose that generating the protease may play a significant role in the pathogenesis of candidemia produced by Candida spp. It has been testified that more than 90% of Candida spp isolates proteinase products 33. Proteinase production was identified in 74.56% of Candida spp. It was also testified that 88% of Candida spp. isolated from blood-linked intense proteinase action.
Moreover, Candida spp. atmospheric environments did not damage isolates testifying strong proteinase action. The alterations between studies may include product from differences in the sources of incubation, isolates and times34.
Sachin et al. (2012) 35 reported that 94.8% of C. albicans samples presented hemolysis activity, whereas hemolysis activity of additional non-C.albicans extended from 7% to 60%; similarly, Sathiya et al. (2015) 36 described 100% of Candida spp. isolates exhibited β-hemolytic.
Form biofilms are associated with pathogenicity and should be considered an important virulence determinant during candidiasis. Biofilms may help fungi maintain the role of commensal and pathogen by evading host immune mechanisms, resisting antifungal treatment, and withstanding the competitive pressure from other organisms37.
Our results are in good agreement with Khan's et al. results (2012) 38, where amphotericin B and Fluconazole showed vigorous antifungal activity against Candida due to their MIC standards of under 100 μg/ml. Also, the antifungal proved to be an active inhibitor against C. glabrata 39. According to Hafidh et al. (2011) 40, the MFC/MIC relation is used to identify the influence of the antifungal effect against a specific pathogen. When the percentage of MFC:MIC result is between 1:1 and 2:1, the biochemical analysis measured fungicidal. In addition, Mohamadi et al. (2014) 41 also testified the fungicidal action of strain, using the destroy time technique in C. albicans and expending agar disc diffusion test, for example C. albicans, C.tropicalis, and C. glabrata. Fungicidal action is clinically more significant than fungistatic action. The prophylactic usage of fungistatic treatments has been related to an increased rate of innate or acquired immunity in clinical isolates 24-44.
CONCLUSIONS
Candida samples vary in their ability to form virulence factors, such as the production of phospholipase, proteinase, biofilms, and hemolysis when taken from leukemia patients. Candida spp samples were more sensitive to Fluconazole followed by Flucytosine, Amphotericin B, Voriconazole, Caspofungin, and Micafungin.
Funding
Not applicable
Acknowledgments
The authors like to thank the Department of Molecular and Medical Biotechnology at the College of Biotechnology/Al-Nahrain University and the Department of Chemistry at the College of Science/Al-Nahrain University for partially supporting this work.
Conflicts of Interest
The authors declare no conflict of interest
REFERENCES
1. Saikkonen K. Forest structure and fungal endophytes. Fungal Biol. Rev. 2007; 21: 67–74. doi:10.1016/j.fbr.2007.05.001
2. Risan M H. Molecular Identification of Yeast Candida glabrata from Candidemia Patients in Iraq. Iraqi J. Sci. 2016; 808-813.
3. Mei-Yin L, Jen-Fu H , Shih-Ming C , Hsyuan W, Hsuan-Rong H, Ming-Chou C, Ren-Huei F, Ming-Horng T. Risk Factors and Outcomes of Recurrent Candidemia in Children: Relapse or Re-Infection. J. Clin. Med. 2019; 8: 99. doi:10.3390/jcm8010099
4. Cleveland A A, Harrison L H, Farley M M, Hollick R, Stein B, Chiller T M , Lockhart S R, Park B J. Declining incidence of candidemia and the shifting epidemiology of Candida resistance in two US metropolitan areas 2008–2013: Results from Population-Based Surveillance. Microb. Pathog 2018; 117: 128-13. https://doi.org/10.1371/journal.pone.0120452
5. Blot S I, Vandewoude K H, Hoste E A. Colardyn F A. Effects of nosocomial candidemia on outcomes of critically ill patients. A.M. J. Med. 2002; 113: 480-485. doi: 10.1016/s0002-9343(02)01248-2
6. Ruan S Y, Hsueh P R. Invasive candidiasis: an overview from Taiwan. J. Formos. Med. Assoc.2009; 108: 443-451. doi: 10.1016/S0929-6646(09)60091-7
7. Chih-Cheng L, Wang C Y, Wei-Lun Liu W L, Huang, Y T, Hsueh P R. Time to positivity of blood cultures of different Candida species causing fungaemia. J. Med. Microbiol. 2012; 61: 701-704. DOI 10.1099/jmm.0.038166-0
8. Mohandas V, Ballal M. Proteinase and phospholipase activity as virulence factors in Candida species isolated from blood. Rev Iberoam Micol 2008; 25: 208-10. doi: 10.1016/s1130-1406(08)70050-0
9. Zaoutis T E, Argon J, Chu J, Berlin J A, Waish, T J, Feudtner C. The epidemiology and attributable outcomes of candidemia in adults and children, hospitalized in the United States: a propensity analysis. Clin. Infect. Dis. 2005; 41 (9): 1232-1239. doi: 10.1086/496922
10. Labelle A J, Micek S T, Roubinian N, Koilef M H . Treatment-related risk factors for hospital mortality in Candida bloodstream infections. Crit.Care Med. 2008; 36 (11): 2967-2972. DOI: 10.1097/CCM.0b013e31818b3477
11. Costa C R, Passos X S, Hasimoto L K, Lucena F O, Silva M. Differences in exoenzyme P. production and adherence ability of Candida spp. isolates from catheter, blood and oral cavity. Rev. Inst. Med. Trop. Sao Paulo 2010; 52 (3): 139-143. http://dx.doi.org/10.1590/S0036-46652010000300005
12. Suleyman G, Alangaden G J. Nosocomial fungal infections: epidemiology, infection control, and prevention. Infect. Dis. Clin. North Am. 2016; 30: 1023-1052. doi: 10.1016/j.idc.2010.11.003
13. Rodrigues C F, Silva S, Henriques M. Candida glabrata: A review of its features and resistance. Eur. J. Clin. Microbiol. Infect. Dis. 2014; 33: 673–688. doi: 10.1007/s10096-013-2009-3
14. Garcia-Cuesta C, Sarrion-Perez M G, Bagan J V. Current treatment of oral candidiasis: A literature review. J. Clin. Exp. Dent. 2014; 6: 576–582. doi:10.4317/jced.51798
15. Colle J G, Fraser A G, Marmion B P, Simmons A. Pactical medical microbiology.14th ed. Curchill living stone 1996; USA.
16. Emmons C W, Binford C H, Uts J P, Kwonchung, K J. Medical Mycology. 1977; 3rd Ed. Lea and Febiger. Philadelphia.
17. Willinger B, Hillowoth C, Selitsch B, Manafi M. Performance of Candida ID, a new chromogenic medium for presumptive identification of Candida species, in comparison to CHROMagar Candida, J. Clin. Microbiol 2001; 39: 3793-3795. DOI: 10.1128/JCM.39.10.3793–3795.2001
18. Murray P R. Manual of Clinical Microbiolog. 9th Ed. American Society for Microbiology 2007; Washington, D.C.
19. Janaina C O, Duque C, Flávia S, Iza T A, José F, Reginaldo B. Candida spp. in periodontal disease: a brief review. J. Oral Sci. 2010; 52 (2): 177-185. doi: 10.2334/josnusd.52.177
20. Deepa K, Jeevitha T, Michael A. In vitro evaluation of virulence factors of Candida species isolated from oral cavity. J. Microbiol. Antimicrob 2015; 7(3):28-32. https://doi.org/10.5897/JMA2015.0337
21. Mohandas V, and Ballal M, . Proteinase and phospholipase activity as virulence factors in Candida species isolated from blood. Rev Iberoam Micol., 2008; 25: 208-10.
22. Akcağlar S, Ener B, Tore O. Acid proteinase enzyme activity in Candida albicans strains: a comparison of spectrophotometry and plate methods. Turk. J. Biol. 2001; 67-559:35. doi:10.3906/biy-1002-39
23. Yenişehirli G, Bulut Y, Tunçoglu E, . Phospholipase proteinase and hemolytic activities of Candida albicans isolates obtained from clinical specimens. Mikrobiyol Bul. 2010; 44: 71-7.
24. Gültekin B, Eyigör M, Tiryaki Y, Kırdar S, Aydın N, . Investigation of antifungal susceptibilities and some virulence factors of Candida strains isolated from blood cultures and genotyping by RAPD-PCR. Mikrobiyol Bul. 2011; 45: 306-17.
25. Melek I, Mustafa A A, Ayse N K, Erkan Y, Omar E, Suleiman D, Gonca D. Investigating virulence factors of clinical Candida isolates in relation to atmospheric conditions and genotype. Turk .J. Med. Sci. 2012; 42(2):1476-1483. doi:10.3906/sag-1204-119
26. Naveen S, Deepak M, Divya D, Savita S. Evaluation of congo red agar for detection of biofilm production by various clinical Candida isolates. J. of Evolution of Med. and Dent. Sci 2014; 3 (59): 2278-4748. DOI: 10.14260/jemds/2014/3761
27. Andrew M B, Fraser M, Michael D P, Szekely A, Houldsworth M, Patterson Z, Elizabeth M J. MIC Distributions and Evaluation of Fungicidal Activity for Amphotericin B, Itraconazole, Voriconazole, Posaconazole and Caspofungin and 20 Species of Pathogenic Filamentous Fungi Determine Using the CLSI Broth Microdilution Method. J. Fungi 2017; 3: 27. doi: 10.3390/jof3020027
28. Rex J H, Pfaller M A, Walsh T J, Chaturvedi V, Espinel-Ingroff A et al. Antifungal susceptibility testing: Practical aspects and current challenges. Clin. Microbiol. Rev. 2001; 14: 643-658. DOI: 10.1128/CMR.14.4.643–658.2001
29. Ghelardi E, Pichierri G, Castagna B, Barnini S, Tavanti A, Campa M. Efficacy of Chromogenic Candida Agar for isolation and presumptive identification of pathogenic yeast species. Clin Microbiol Infect. 2007; 1469-0691. doi: 10.1111/j.1469-0691.2007.01872.x
30. Wisplinghoff H, Bischoff T, Tallent S M, Seifert H, Wenzel R P, Edmond M B. Nosocomial bloodstream infections in US hospitals: analysis of 24,179 cases from a prospective nationwide surveillance study. Clin. Infect. Dis. 2004; 39: 309-317. doi: 10.1086/421946
31. Motta-Silva A C, Aleva N A, Chavasco, J K, Armond M C, França J P, Pereira L J . Erythematous Oral Candidiasis in Patients with Controlled Type II Diabetes Mellitus and Complete Dentures, Mycopathologia. 2010; 169: 215-223. https://doi.org/10.1007/s11046-009-9240-6
32. Chakrabarti A, Shivaprakash M, Ghosh A. Standard Operating procedures, Mycology Laboratories. Indian Council of Medical Research 2016; 5-47.
33. Baillie G S, Douglas L J. Candida biofilm and their susceptibility to antifungal agents. Methods Enzymol 1999; 310: 644-56. doi: 10.1016/s0076-6879(99)10050-8
34. Silva J O F S, Lavrador M A, Candido R C. Performance of selective and differential media in the primary isolation of yeasts from different biological samples.Mycopathologia. 2004; 151(1):29-36. https://doi.org/10.1023/B:MYCO.0000012223.38967.7d
35. Sachin C D, Ruchi K, Santosh S. In vitro evaluation of proteinase, phospholipase and haemolysin activities of Candida species isolated from clinical specimens. Int. J. Med. Bio Res. 2012; 1(2):153-157. DOI: 10.14194/ijmbr.1211
36. Sathiya T, Arul Sheeba M S, Moorthy K, Punitha T, Vinodhini R, Saranya, A S. Candida albicans non-albicans species: Astudy of biofilm production and putative virulence properties. J. Harmo. Res. Pham. 2015; 4(1): 64-75. DOI: 10.1007/s11046-013-9638-z
37. Khan S M A, Malik A, Ahmad I. Anti-candidal activity of essential oils alone and in combination with amphotericin B or Fluconazole against multi-drug resistant isolates of Candida albicans. Med Mycol 2012; 50: 33 - 42. doi: 10.3109/13693786.2011.582890
38. Espinel-Ingroff A, Chaturvedi V, Fothergill A, Rinaldi M G. Optimal testing conditions for determining MICs and minimum fungicidal concentrations of new and established antifungal agents for uncommon molds: NCCLS collaborative study. J. Clinic Microbiol 2002; 40: 3776 - 3781. DOI: 10.1128/JCM.40.10.3776–3781.2002
39. Mohamadi J, Motaghi M, Panahi J, Havasian M R, Delpisheh A, Azizian M, Pakzad I. Anti-fungal resistance in candida isolated from oral and diaper rash candidiasis in neonates. Bioinformation 2014; 10:667-70. DOI: 10.6026/97320630010667
40. Hafidh R R, Abdulamir A S, Vern L S, Bakar F A, Abas F, Jahanshiri F, Sekawi Z. Inhibition of growth of highly resistant bacterial and fungal pathogens by a natural product. Open Microbiol. J. 2011; 5: 96 -106. doi: 10.2174/1874285801105010096
41. Monk B C, Goffeau A. Outwitting multidrug resistance to antifungals. Science 2008; 321: 367 - 369. DOI: 10.1126/science.1159746
42. Luksamijarulkul P, Aiempradit N, Vatanasomboon P. Microbial contamination on used surgical masks among hospital personnel and microbial air quality in their working wards: A hospital in Bangkok. Oman Med J 2014; 29(5):346-350. DOI: 10.5001/omj.2014.92
43. Mohammad T, Risan M, El-Hiti G, Ahmed D, Yousif E. Successful in-vivo treatment of mice infected with Candida glabrata using silver nanoparticles. Bionatura 2020, 5(4), 1340–1345. DOI. 10.21931/RB/2020.05.04.10
Received: 4 April 2021
Accepted: 25 June 2021
Teeba Hashim Mohammed 1, Mohsen Hashim Risan 1, Mohammed Kadhom2, Emad Yousif3,*
1 College of Biotechnology, Al-Nahrain University, Baghdad, Iraq
2 Department of Renewable Energy, College of Energy and Environmental Sciences, Alkarkh University of Science, Baghdad, Iraq
3 Department of Chemistry, College of Science, Al-Nahrain University, Baghdad, Iraq
* Corresponding author [email protected]