2022.07.03.38
Files > Volume 7 > Vol 7 No 3 2022
NOD1/CARD4(G796A) and NOD2/CARD15(R702W, G908R and L1007fsinC) polymorphisms associated with Crohn's disease in Iraqi patients

Adnan Fayadh Sameer*1 , Abed Hassan Barraj2, Hayder Jamaal Mahmood3.
, Abed Hassan Barraj2, Hayder Jamaal Mahmood3.
1,2, Department of Biology, collage of Science, University of Baghdad3 Gastroenterologist and Hepatologist, Gastrointestinal of the hospital, City of medicine.
*Corresponding author: Adnan Fayadh Sameer. E-mail: Adnanfayadh80@gmail .com ,
Available from: http://dx.doi.org/10.21931/RB/2022.07.03.38
ABSTRACT
Inflammatory bowel disease (IBD) applies to two main forms of chronic relapsing inflammatory intestinal disorders: Crohn's disease (CD), Ulcerative colitis (UC). CD requires an irregular immune reaction that induces intense inflammation. The cause of CD disease is not yet fully known; previous research, however, indicated inflammation of the intestines elevated or continues due to inappropriate immune responses due to associations between genetic factors, intestinal microbiota, and environmental factors contributing to the production of IBD. This study aimed to investigate predisposing genes, single nucleotide Polymorphisms (SNPs) NOD1/CARD4 and NOD2/CARD15) with CD in Iraqi patients. The common NOD1 (G796A) SNP and NOD2 SNPs R702W, G908R and L1007fsinC for NOD2 SNPs were selected. Thirty Iraqi citizens with a recognized diagnosis of CD and twenty apparently healthy controls were included in the study from November 2019 to December 2020; the common NOD1 and NOD2 polymorphisms have been screened by the polymerase chain reaction/restriction analysis length polymorphism (PCR/RFLP). The results of the current investigation for NOD1 polymorphism in studied patients and controls, the allelic and genotypic data show a highly significant association of G796A SNPs in the NOD1 with Crohn's disease, GA percentage was 56.67% in patients as compared to controls genotype was (0.00%).
Furthermore, the G allele was more common in Crohn's patients than the A allele 0.72 vs. 0.28. Also, the allelic and genotypic frequency distribution of the studied NOD2 SNPs in the current study were (R702W, G908R, and L1007fs) in Iraqi patients, and controls revealed a highly significant connection between the G908R SNP with Crohn's disease susceptibility. The proportion of the genotype GC was 30% in patients while 0% in the control group, the frequency of the G allele was 0.85 vs 0.15 respectively, which was more than the frequency of the A allele. There were no significant changes in genotypic and allelic frequencies of the R702W and L1007fs SNPs in Iraqi Crohn's disease patients. The present study concluded that the NOD1 SNP of allelic and genotypic data show a highly significant association of G796A with a predisposition to Crohn's disease in Iraqi patients. And the NOD2 SNPs of G908R were also revealed to be highly effective. While the other studied SNPs were R702W and L1007fsinsC of NOD2, which showed no significant changes in the allelic and genotypic frequencies of the SNPs with Crohn's disease Iraqi patients.
Keywords: Inflammatory bowel disease, Crohn's disease, NOD1/CARD4, NOD2/CARD15, polymorphisms.
INTRODUCTION
Crohn's disease (CD) can be defined as a common inflammatory bowel disease (IBD) type; one other IBD form, Ulcerative colitis (UC) induces chronic inflammation (transmural inflammation). In contrast to the CD that may impact any digestive system part, the UC typically causes inflammation in the colon only; CD is a long-lasting (i.e., chronic) and complex condition that mainly impacts the digestive system 1. This disease requires an irregular immune reaction that induces intense inflammation. It more frequently affects intestinal walls, especially in the small intestine's lower part (ileum) and in large intestine portions (i.e., colon); inflated tissues grow thicker and get swollen. The inside becomes swollen, and open sores (ulcers) may form the inner digestive system's surfaces 2. Crohn's disease most often develops in the late teens or the 20s, but this disease could affect people of any age. Symptoms and signs appear to outbreak many times during a lifetime. This disorder's most common symptoms include stomach pain and cramping, persistent diarrhea, weight loss, fever and appetite loss. Any people with CD get blood in the stool with inflamed tissues in the Intestines; persistent bleeding may lead to (anemia). In certain situations, CD may result as well in causing inflammations in the eyes, skin, or joints 3,4.
The cause of IBD is not yet fully known; previous studies indicated the inflammation of the intestines elevated or continues because of inappropriate immune responses due to associations between genetic factors, intestinal microbiota, and environmental factors contributing to the production of IBD. Results of previous studies support the speculation that genetic factors are involved in IBD; the frequency and incidence of IBD vary geographically and ethnically 5,6.
The incidence of CD in Iraq has been rising in the last years 16. In addition, the incidence of IBD seems to be growing in Egypt 15. The documented data shows, too, that there has been an amazingly increasing trend in the incidence rate of CD in Saudi Arabia 12; in Kuwait, both the prevalence and incidence of CD are growing at a rate comparable to that seen in Western countries 13,14. Crohn's disease is most prevalent in North America, northern Europe, and New Zealand, between the ages of 15- 60. Since 1990, the highest reported prevalence of IBD has been observed in the industrialized countries of 322 CD patients per 100,000 persons in Germany 7,8. The highest incidences of IBD are reported in European countries and North America (15.4 and 23.82 per 100,000 person-years for CD in Italy and Canada, respectively 8. Conversely, progressively increasing incidences were noticed in Asia and the Middle East, reaching rates of 5 per 100,000 person-years for CD 9. Northern Europeans and Jews of (Ashkenazi) origin have a high frequency (Incidence 3.2/1000) as opposed to substantial infrequent prevalence of Asians, Africans and South Americans 10. The latest reports, however, have shown a significant rise in incidence in increasingly industrializing Asia, Africa, and Australasia11.
About a hundred IBD-associated gene polymorphisms have identification; the CD tends to have a genetic correlation of phenotypes. Specifically, nucleotide binding and oligomerization domains containing protein 2/Caspase recruitment domain family member 15 (NOD2/CARD15) and nucleotide binding and oligomerization domains containing protein 1/Caspase recruitment domain family member 4 (NOD1/CARD4) polymorphisms were shown to be correlated with CD phenotypes associated with those diagnosed at a younger age, 17,18. Nucleotide-binding and oligomerization domains containing protein (NOD) can detect intracellular muramyl dipeptide (MDP), a component of the bacterial wall that is ubiquitously present in bacterial peptidoglycan can 19. Upon ligand activation, NOD mediates an innate immune response that activates as a pro-inflammatory response in patients with persistent inflammatory conditions such as CD have been shown to have NOD2 polymorphism or altered expression 20. At this point, evaluating for genetic mutations in CD still remains a research tool, not yet proven to be of clinical benefit for diagnosis, treatment or prognosis. The current study aims to Investigate the predisposing genes NOD1 and NOD2 polymorphisms with CD in Iraqi patients, three common single nucleotide Polymorphisms (SNPs) were selected (Arg702Trp (R702W), Gly908Arg (G908R) and Leu1007fsinsC (L1007fsinC) for NOD2 and Glycin796Alanine (G796A) SNP for NOD1.
MATERIALS AND METHODS
Tissue biopsies of 30 cases with a recognized diagnosis of Crohn's disease. Additionally, 20 cases as control ranged from 9-55(±34.78) years in the Patients and Control group(apparently healthy individuals). From November 2019 to December 2020, Biopsies were collected from Gastro-Enterology and Hepatology Teaching Hospital in Baghdad.
Therefore, one endoscopic tissue biopsy was collected from each Crohn's disease case; the biopsy was placed in normal saline for single nucleotide polymorphism (SNP) detection. All SNPs were genotyped by polymerase chain reaction (PCR) - restriction fragment polymorphism analysis (PCR-RFLP. In this study, RFLP is a method that uses SNP to exploit variations in homologous DNA sequences. SNP for NOD1 to distinguish G796A (E266K) (rs2075820). Furthermore, three single nucleotide polymorphisms (SNPs) for NOD2 were chosen: (R702W, G908R, and L1007fsincC) rs (2066844, rs2066845, and rs2066847) respectively.Table 1.
Steps of RFLP Analysis:
Step1 Isolating the DNA.
Step2 Performing PCR.
Step3 Performing the Restriction Digestion.
Step4 Preparing the Sample for Analysis.
Step5 Performing the Electrophoresis.
Step6 Analyzing the Data.

Table 1. The sequence of primers used in this study.
Statistical analysis
The Statistical Analysis System- SAS (2012) software has been utilized to detect the effects of various factors in the study's parameters. T-test has been utilized for the significant comparison between the mean values. The Chi-square test has been used to significantly compare the percentage (0.05 and 0.01 probability in this study. The allelic frequency and equilibrium of the studied genes were extracted according to the Hardy-Weinberg equation.
RESULTS
Frequency of NOD1/CARD4 gene G796A (rs2075820) polymorphisms
Allelic and genotypic data from this study show a highly significant association of G796A rs2075820 SNPs in the NOD1 gene with CD. The SNP G796A carriage variant for the NOD1 gene was an important risk factor for CD. The chi-square value was 11.728, a significant value for the genotype GA. The percentage of heterozygous genotype GA was 56.67% compared to seemingly healthy controls; genotype GA was not detected, while genotype AA was not detected in patients and control. Furthermore, allele G was considerably more common in Crohn's patients than allele A (0.72 vs. 0.28) (P≤0.01) table (2). Figures (1 and 2) show results for NOD1 SNP G796A genotyping.

Table 2. Genotype and Allele frequency of NOD1- G796A rs2075820 SNP in Iraqi Patients with CD

Figure 1 Agarose gel electrophoresis (2%) with RedSafe stain® at 80V for NOD1 (G796A) SNP rs2075820. PCR product length 379bp.

Figure 2. Agarose gel electrophoresis (3%) with RedSafe stain® at 80V for NOD1 (G796A) SNP rs2075820. with an expected size of digested fragment length by restriction Aval enzyme;(209bp and 170bp for genotype G/G WT. And (379bp,209bp and 170bp for G/A allele).
Distribution of the CD-associated NOD2 SNPs (R702W, G908R, and L1007fs)
In Iraqi patients and controls, the allelic and genotypic frequency distribution of the three primary CD-associated NOD2 SNPs (R702W, G908R, and L1007fs). Revealed a highly significant connection of only the G908R (rs2066845) SNP with CD susceptibility, the genotype of G908R was detected by chi-square value was 8.923, which is a highly significant value for the genotype GC. The percentage of heterozygosity for the genotype GC was 30% in patients and not detected in the control group, while genotype CC was not detected in patients and control. The frequency of the allele G to G908R SNP was 0.85, which was more than the frequency of the allele A, which was 0.15 (P≤0.01) table (3), figures (5 and 6). There were no significant changes in genotypic and allelic frequencies of the R702W rs2066844 and L1007fs rs2066847 SNPs in CD patients (figures3 4, and 7,8).

Table 3. Genotype and Allele frequency of NOD2 (G908R) rs2066845 in Patients and Control groups

Figure 3. Agarose gel electrophoresis (2%) with RedSafe® stain at 80V for NOD2 (R702W) SNP rs2066844, PCR product length 185bp.

Figure 4. Agarose gel electrophoresis (3%) with RedSafe® stain at 80V for NOD2 (R702W) SNP rs2066844 with an expected digested fragment length by restriction Mspl enzyme (76, 54, 35 bp) for genotype C/ C (WT.).

Figure 5. Agarose gel electrophoresis (2%) with RedSafe® stain at 80V for NOD2 (G908R) SNP rs2066845 with PCR product length 163bp.
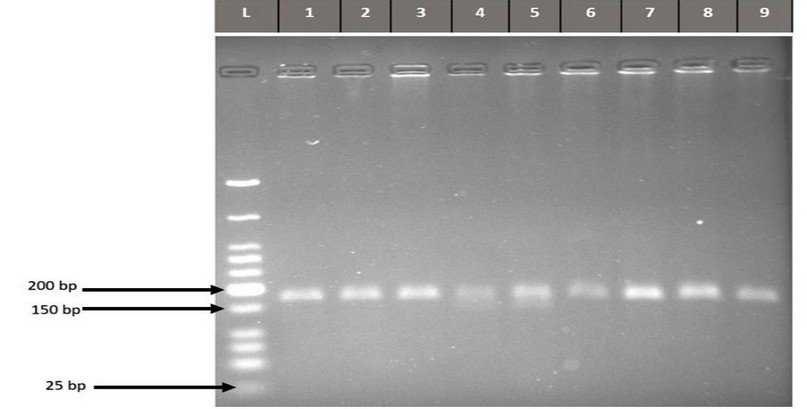
Figure 6. Agarose gel electrophoresis (3%) with RedSafe® at 80V for NOD2 (G908R) SNP rs2066845 with an expected digested fragment length by restriction Hhal enzyme (163bp for genotype G/G (WT.), 136bp for G/C bp).

Figure 7. Agarose gel (2%) stained by RedSafe® and 80V electrophoresis for NOD2 (3020 insC) 1007fs SNP rs2066847 with PCR product length 514bp

Figure 8. Multiple alignments (NOD2 )3020insC SNP rs2066847 for DNA sequences table related to differences between samples.
DISCUSSION
The current study is one of the new studies to examine the incidence of the G796A mutation in CD patients in Iraq. Our findings imply that the presence of this SNP is a substantial susceptibility factor for CD in the Iraqi population, which is consistent with previous findings indicating the presence of the NOD1 (G796A) SNP enhances susceptibility to CD in the Hungarian population 21. In dissimilarity to the investigation of NOD1 (G796A) rs2075820 (G>A) in Turkish CD patients, which revealed no significant association between the SNP and the onset of CD 40, the current study found a significant association between the NOD1 (G796A) rs2075820 SNP and the onset of CD. The allele A has been proposed to reduce helix-formatting capability and influence ATP binding affinity. As a result, NOD1 polymorphism may not be directly associated with CD beginning but rather through a convoluted pathway initiated by infection 21. We believe that changing a negatively charged amino acid to a positively charged one and a probable alteration in the orientation of lateral chains at residues 266 could have an impact on the interaction of effector proteins and adaptor molecules with the central nucleotide-binding domain termed (NACHT) domain 23. There are no exact data to show how the NOD1 polymorphism affects the NOD1 function. Still, our findings suggest that changing negatively-charged glutamine to positively-charged lysine may cause a severe change in the structure or regulation of the NOD1 protein, altering reactivity to some pathogenic bacteria or the nature of downstream inflammatory pathways. NOD1 polymorphisms were also frequently associated with inflammatory responses following Helicobacter pylori infection, such as duodenal ulcer and gastritis 24. As a result, NOD1 polymorphism may not be directly related to the onset of CD but rather through a complicated mechanism triggered by infection. In the current investigation, we attempted to establish a link between IBD, CD, and the three primary variants in the coding revealed that NOD2/CARD15 gene polymorphisms explain roughly 20% of the genetic predisposition to CD in US. and European populations 25. Several investigations, however, have demonstrated that NOD2/CARD15 gene polymorphisms are not illness factors in Asian populations. Some of these patients–control investigations on Japanese, Chinese, and Korean populations 26,27. The G908R rs2066845 G>C SNP variants Heterozygous genotype GC was observed in patients and not detected in the healthy control group; the G908R polymorphism plays an important risk for CD 28. And the frequency of the R702W rs2066844 C > T and 3020insC/1007fs rs2066847 C>G, A, T SNPs variant genotype was not detected, to be 0.0 percent in CD patients for each two SNPs. Although no significant association was found between these R702W and 3020insC/1007fsSNPs variations and CD, the findings of this study revealed the presence of the NOD2/CARD15 and G908R SNP gene variants in the Iraqi population. This G908R SNP is a genetic susceptibility factor for Crohn's disease in Iraq, despite being absent in most Asian and Turkish populations 40. The absence of the NOD2 G702W rs 2066844 and 3020insC (1007fs) rs2066847 SNPs in CD patients show that these variants are not associated with IBD; absent genotype variation in different geographical regions may be due to the different ethnicities and environmental factors of the populations studied. The current results are similar to the previous genetic studies in Asia have revealed that G908R SNP is a common mutation in gene NOD2/CARD15 and is associated with the risk of CD in East Asian populations such as Japan, Korea, and China 8,29. except for mutations G702W and 3020insC (1007fs), unrelated to CD in the Iraqi population. Carrying NOD2 mutations conferred a high chance of developing CD, as expected. However, this was neither essential nor sufficient for CD development. The three NOD2 mutations did not play an equivalent role in CD susceptibility. In other patient population investigations, the presence of R702W was associated with the highest risk of CD. This mutation, however, was not linked to CD in Galician, Finnish, or Scottish populations 30. So, comparable to the current study's findings in the Iraqi population. While L1007finsC polymorphism was the strongest CD connection in various familial and non-familial studies (22). However, in the current investigation, this was not the case. The current investigation found no link between the NOD2/CARD15, R702W, and 3020insC/1007fs SNPs with CD in Iraqi Patients. Because CD is recognized as a disease with numerous etiologies, including various genetic disorders, the predisposing genetic factors in CD may differ amongst populations. NOD2 gene mutations may thus result in the immune system's failure to manage the bacterial infection and the development of chronic inflammation 31. These findings are discordant with those described in prior European research and other North African studies 32,33. The common connection of NOD2 mutations with CD and IBD 34, 35, has been largely repeated 36, but not universally 37. Particularly in North African populations 38, 39. Because of genetic variability, various genes in different individuals are thought to cause hereditary susceptibility to the disease. Because of this genetic variability, the effect of a single gene that is connected with CD in one community may not be observed in another. So the studies may contradict each other 40.
CONCLUSION
Finally, the Conclusion from current data indicates that these R702W and 3020insC/1007fs SNPs are not polymorphic in Iraqi population samples.
Acknowledgment: Thanks going for all who support us.
The conflict between authors: No conflict
Funds: self by authors
REFERENCES
(1) Lightner AL, McKenna NP, Alsughayer A, Loftus EV Jr, Raffals LE, Faubion WA, et al. Anti-TNF biologic therapy does not increase postoperative morbidity in pediatric Crohn's patients. J Pediatr Surg [Internet]. 2019;54(10):2162–5. Available from: http://dx.doi.org/10.1016/j.jpedsurg.2019.01.006
(2) Marazuela GP, López-Jurado A, Vicente BA. Acute abdominal pain in patients with Crohn's disease: what urgent imaging tests should be done? Radiologia. 2019;61(4):333–6.
(3(Aksan A, Farrag K, Stein J. An update on the evaluation and management of iron deficiency anemia in inflammatory bowel disease. Expert Rev Gastroenterol Hepatol [Internet]. 2019;13(2):95–7. Available from: http://dx.doi.org/10.1080/17474124.2019.1553618
(4) Hwang JH, Yu CS. Depression and resilience in ulcerative colitis and Crohn's disease patients with ostomy. Int Wound J [Internet]. 2019;16 Suppl 1:62–70. Available from: http://dx.doi.org/10.1111/iwj.13076
(5) Thia KT, Loftus EV Jr, Sandborn WJ, Yang S-K. An update on the epidemiology of inflammatory bowel disease in Asia. Am J Gastroenterol [Internet]. 2008;103(12):3167–82. Available from: http://dx.doi.org/10.1111/j.1572-0241.2008.02158.x
(6) de Souza HSP, Fiocchi C. Immunopathogenesis of IBD: current state of the art. Nat Rev Gastroenterol Hepatol [Internet]. 2016;13(1):13–27. Available from: http://dx.doi.org/10.1038/nrgastro.2015.186
(7) Hein R, Köster I, Bollschweiler E, Schubert I. Prevalence of inflammatory bowel disease: estimates for 2010 and trends in Germany from a large insurance-based regional cohort. Scand J Gastroenterol [Internet]. 2014;49(11):1325–35. Available from: http://dx.doi.org/10.3109/00365521.2014.962605
(8) Ng SC, Shi HY, Hamidi N, Underwood FE, Tang W, Benchimol EI, et al. Worldwide incidence and prevalence of inflammatory bowel disease in the 21st century: a systematic review of population-based studies. Lancet [Internet]. 2017;390(10114):2769–78. Available from: http://dx.doi.org/10.1016/s0140-6736(17)32448-0
(9) Molodecky NA, Soon IS, Rabi DM, Ghali WA, Ferris M, Chernoff G, et al. Increasing incidence and prevalence of the inflammatory bowel diseases with time, based on systematic review. Gastroenterology [Internet]. 2012;142(1):46-54.e42; quiz e30. Available from: http://dx.doi.org/10.1053/j.gastro.2011.10.001
(10) Coward S, Clement F, Benchimol EI, Bernstein CN, Avina-Zubieta JA, Bitton A, et al. Past and future inflammatory bowel disease burden based on population-based data modeling. Gastroenterology [Internet]. 2019;156(5):1345-1353.e4. Available from: http://dx.doi.org/10.1053/j.gastro.2019.01.002
(11) Ghersin I, Khteeb N, Katz LH, Daher S, Shamir R, Assa A. Trends in the epidemiology of inflammatory bowel disease among Jewish Israeli adolescents: a population-based study. Aliment Pharmacol Ther [Internet]. 2019;49(5):556–63. Available from: http://dx.doi.org/10.1111/apt.15160
(12 ) Al-Nooh BM, Alaslani MH, Almaghamsi A, Basehi M, Mufti F. Crohn's Disease Prevalence and Causes among Saudi Arabia Population. Int J Med Res Prof. 2018;4(1):254–7.
(13) Siddique, I., Alazmi, W., Al-Ali, J., Al-Fadli, A., Alateeqi, N., Memon, A., & Hasan, F. (2012). Clinical epidemiology of Crohn's disease in Arabs based on the Montreal Classification. Inflammatory bowel diseases, 18(9), 1689–1697.
(14) Siddique I, Alazmi W, Al-Ali J, Longenecker JC, Al-Fadli A, Hasan F, et al. Demography and clinical course of ulcerative colitis in Arabs - a study based on the Montreal classification. Scand J Gastroenterol [Internet]. 2014;49(12):1432–40. Available from: http://dx.doi.org/10.3109/00365521.2014.966318
(15) Esmat S, El Nady M, Elfekki M, Elsherif Y, Naga M. Epidemiological and clinical characteristics of inflammatory bowel diseases in Cairo, Egypt. World J Gastroenterol [Internet]. 2014;20(3):814–21. Available from: http://dx.doi.org/10.3748/wjg.v20.i3.814
(16) Hamasur KS. Prevalence of Oral Manifestations of Inflammatory Bowel Disease in Patients Admitted to Sulaymaniyah teaching hospital – Iraq. Al-Kindy Col Med J [Internet]. 2020;16(1):47–53. Available from: http://dx.doi.org/10.47723/kcmj.v16i1.190
(17) Caruso R, Warner N, Inohara N, Nunez G. NOD1 and NOD2:Singaling,Host Defense, and Inflammatory Disease. Immunity. 2014;18(6):898–908.
(18) Zaidi D, Wine E. Regulation of nuclear factor kappa-light-chain-enhancer of activated B cells (NF-κβ) in inflammatory bowel diseases. Front Pediatr [Internet]. 2018;6:317. Available from: http://dx.doi.org/10.3389/fped.2018.00317.
(19) Kawai T, Akira S. The roles of TLRs, RLRs and NLRs in pathogen recognition. Int Immunol [Internet]. 2009;21(4):317–37. Available from: http://dx.doi.org/10.1093/intimm/dxp017.
(20) Negroni A, Pierdomenico M, Cucchiara S, Stronati L. NOD2 and inflammation: current insights. J Inflamm Res [Internet]. 2018;11:49–60. Available from: http://dx.doi.org/10.2147/jir.s137606.
(21) Molnár T, Hofner P, Nagy F, Lakatos PL, Fischer S, Lakatos L, et al. NOD1 gene E266K (G796A) polymorphism is associated with disease susceptibility but not with disease phenotype or NOD2/CARD15 in Hungarian patients with Crohn's disease. Z Gastroenterol [Internet]. 2007;45(05). Available from: http://dx.doi.org/10.1055/s-2007-982693.
(22 ( Heliö T, Halme L, Lappalainen M, Fodstad H, Paavola-Sakki P, Turunen U, et al. CARD15/NOD2 gene variants are associated with familially occurring and complicated forms of Crohn's disease. Gut [Internet]. 2003;52(4):558–62. Available from: http://dx.doi.org/10.1136/gut.52.4.558.
(23) Proell M, Riedl SJ, Fritz JH, Rojas AM, Schwarzenbacher R. The Nod-like receptor (NLR) family: a tale of similarities and differences. PLoS One [Internet]. 2008;3(4):e2119. Available from: http://dx.doi.org/10.1371/journal.pone.0002119.
(24) Kara B, Akkiz H, Doran F, Bayram S, Erken E, Gumurdullu Y, et al. The significance of E266K polymorphism in the NOD1 gene on Helicobacter pylori infection: an effective force on pathogenesis? Clin Exp Med [Internet]. 2010;10(2):107–12. Available from: http://dx.doi.org/10.1007/s10238-009-0077-6.
(25) Hugot J. Inflammatory bowel disease: a complex group of genetic disorders. Best Pract Res Clin Gastroenterol [Internet]. 2004;18(3):451–62. Available from: http://dx.doi.org/10.1016/s1521-6918(04)00009-5
(26) Yamazaki K, Takazoe M, Tanaka T, Kazumori T, Nakamura Y. Absence of mutation in the NOD2/CARD15 gene among483 Japanese patients with Crohn's disease. J Hum Genet. 2002;47:469–72.
(27) Leong RWL, Armuzzi A, Ahmad T, Wong ML, Tse P, Jewell DP, et al. NOD2/CARD15 gene polymorphisms and Crohn's disease in the Chinese population: CROHN'S DISEASE IN THE CHINESE POPULATION. Aliment Pharmacol Ther [Internet]. 2003;17(12):1465–70. Available from: http://dx.doi.org/10.1046/j.1365-2036.2003.01607.x
(28) Adler J, Rangwalla SC, Dwamena BA, Higgins PD. The prognostic power of the NOD2 genotype for complicated Crohn's disease: a meta-analysis. Am J Gastroenterol [Internet]. 2011;106(4):699–712. Available from: http://dx.doi.org/10.1038/ajg
(29) Cheon JH. Genetics of inflammatory bowel diseases: a comparison between Western and Eastern perspectives: Genetics of inflammatory bowel diseases. J Gastroenterol Hepatol [Internet]. 2013;28(2):220–6. Available from: http://dx.doi.org/10.1111/jgh.12053
(30) Núñez C, Barreiro M, Domínguez-Muñoz JE, Lorenzo A, Zapata C, Peña AS. CARD15 mutations in patients with Crohn’s disease in a homogeneous Spanish population. Am J Gastroenterol [Internet]. 2004;99(3):450–6. Available from: http://dx.doi.org/10.1111/j.1572-0241.2004.04066.x
(31) Koning D, Simon HDA, Zeeuwen PL, Schalkwijk J. Pattern recognition receptors in infectious skin diseases. Microbes Infect. 2012;14(11):881–93.
(32) Rehman A, Sina C, Gavrilova O, Häsler R, Ott S, Baines JF, et al. Nod2 is essential for temporal development of intestinal microbial communities. Gut [Internet]. 2011;60(10):1354–62. Available from: http://dx.doi.org/10.1136/gut.2010.216259
(33) Marrakchi R, Bougatef K, Moussa A, Ouerhani S, Khodjet-el-Khil H, Messai Y, et al. 3020insC insertion in NOD2/CARD15 gene, a prevalent variant associated with anti-Saccharomyces cerevisiae antibodies and ileal location of Crohn's disease in Tunisian population. Inflamm Res [Internet]. 2009;58(4):218–23. Available from: http://dx.doi.org/10.1007/s00011-008-8139-x
(34) Rahman P, Bartlett S, Siannis F, Pellett FJ, Farewell VT, Peddle L, et al. CARD15: a pleiotropic autoimmune gene that confers susceptibility to psoriatic arthritis. Am J Hum Genet [Internet]. 2003;73(3):677–81. Available from: http://dx.doi.org/10.1086/378076
(35) Daniil Z, Mollaki V, Malli F, Koutsokera A, Antoniou KM, Rodopoulou P, et al. Polymorphisms and haplotypes in MyD88 are associated with the development of sarcoidosis: a candidate-gene association study. Mol Biol Rep [Internet]. 2013;40(7):4281–6. Available from: http://dx.doi.org/10.1007/s11033-013-2513-7
(36) Hoffmann C, Hoffmann P, Lun A, Büning C, Hiepe F, Scherer HU, et al. Is there a role for mannan-binding lectin in the diagnosis of inflammatory bowel disease? Immunogenetics [Internet]. 2010;62(4):231–5. Available from: http://dx.doi.org/10.1007/s00251-010-0429-0
(37) Gasche C, Nemeth M, Grundtner P, Willheim-Polli C, Ferenci P, Schwarzenbacher R. Evolution of Crohn’s disease-associated Nod2 mutations. Immunogenetics [Internet]. 2008;60(2):115–20. Available from: http://dx.doi.org/10.1007/s00251-008-0274-6
(38) Abida O, Kallel-Sellami M, Joly P, Ben Ayed M, Zitouni M, Masmoudi A, et al. Anti-desmoglein 1 antibodies in healthy related and unrelated subjects and patients with pemphigus foliaceus in endemic and non-endemic areas from Tunisia. J Eur Acad Dermatol Venereol [Internet]. 2009;23(9):1073–8. Available from: http://dx.doi.org/10.1111/j.1468-3083.2009.03265.x
(39) Meddour Y, Chaib S, Bousseloub A, Kaddache N, Kecili L, Gamar L, et al. NOD2/CARD15 and IL23R genetic variability in 204 Algerian Crohn's disease. Clin Res Hepatol Gastroenterol [Internet]. 2014;38(4):499–504. Available from: http://dx.doi.org/10.1016/j.clinre.2014.02.003
(40) Ozen SC, Dagli U, Kiliç MY, Törüner M, Celik Y, Ozkan M, et al. NOD2/CARD15, NOD1/CARD4, and ICAM-1 gene polymorphisms in Turkish patients with inflammatory bowel disease. J Gastroenterol [Internet]. 2006;41(4):304–10. Available from: http://dx.doi.org/10.1007/s00535-005-1780-z
Received: 7 January 2022 / Accepted: 2 May 2022 / Published:15 August 2022
Citation: Sameer A F, Barraj A H, Mahmood H J. NOD1/CARD4(G796A) and NOD2/CARD15(R702W, G908R and L1007fsinC) polymorphisms associated with Crohn's disease in Iraqi patients. Revis Bionatura 2022;7(3) 38. http://dx.doi.org/10.21931/RB/2022.07.03.38