2022.07.04.67
Files > Volume 7 > Vol 7 No 4 2022

Jaleel Hussein Al-Obaidi1,2*
1 Al-kindy College of Medicine, Baghdad University, Iraq; 2 Medical director of Al-Shafa private hospital, Iraq;
*Correspondence author: [email protected] ; Tel.: 009647722221381
Available from: http://dx.doi.org/10.21931/RB/2022.07.04.67
ABSTRACT
Appendicular mass is a well-known complication of acute appendicitis. It is conventionally treated conservatively, followed by interval appendectomy. This study aimed to determine the feasibility and safety of an early appendectomy in appendicular mass. Patients and methods: The analysis was performed at the Department of Surgery Al-Shafaa Hospital Diyala from March 2017 to December 2021. The patients with appendicular mass (n = 100) were included in this study. Patients were divided into two groups, viz. group A (n = 50) and group B (n = 50), regardless of age and gender. After preliminary investigations, appendectomy was performed in group A patients immediately. Group B patients were initially treated with the conventional procedure followed by interval appendectomy. Patient compliance, readmission and overall expenses were recorded for both groups. Results: A total of 60 (64%) males and 40 (40%) females with a mean age of 25.09 years (Range 8-44 years) are included in the study population. Post-operative wound sepsis occurred in 3 (6%) patients in group A. Treatment failure, patient compliance, readmission and overall expenses occurred in group B patients. Early appendectomy was a safe and superior option in patients with appendicular mass compared to conventional treatment.
Keywords: Acute appendicitis. Appendicular Mass, Conservative management, immediate surgery.
INTRODUCTION
The most frequent cause of acute abdomen in teenagers needing surgery is acute appendicitis. 1. Patients admitted late in the acute appendicitis course showed complications such as developing an inflammatory mass in the right iliac fossa2. The inflamed appendix, omentum, and intestinal loops make up this swelling of inflammation. The treatment of appendicular mass is controversial; however, several management options exist for appendicular mass2-5. Traditionally, these patients are managed conversantly, followed by interval appendectomy after 4-6 weeks. It is believed that early appendectomy is hazardous, time-consuming and may lead to life-threatening complications such as faecal fistula6, 7. The need for interval appendectomy has also been questioned8, 9. The initial conventional approach claims to be a lower complication rate than the early operative approach10. Several studies reported that the immediate appendectomy claims to have an early recovery and complete cure during admission11-13. The current study aimed to compare patients treated alternatively and then had interval appendectomy to assess the feasibility and safety of immediate appendectomy in the treatment of appendicular mass in the Iraqi population.
MATERIALS AND METHODS
Patients and Methods
A prospective comparative study was conducted at the Department of Surgery, Al-Shafa private hospital, from March 2017 to December 2021. The patients (n=100) with appendicular mass were induced in this study. All the patients were clinically evaluated. Their blood chemistry, urine analysis, abdomen ultrasound, and plain abdomen x-ray were investigated. The patients were divided into two groups viz. Group A and group B. Treatment options were informed to each patient, and consent was taken.
Operational procedure
Group A was operated on within 24 hours of admission. Patients in group B were kept on conventional treatment comprising hospitalization with intravenous fluids and broad-spectrum antibiotics such as Cefuroxime, Metronidazole and analgesics. The mass progress and the vitals were recorded regularly to monitor the response to conventional treatment. The patients in group B were discharged after complete resolution of the acute inflammatory mass and re-admitted after 6-8 weeks for interval appendectomy.
Studied parameters
The variables studied in both groups included operative difficulties, total operating time, operative and postoperative complications, total duration of hospital stay and patient compliance.
RESULTS
The study included 60 (60 %) males and 40 (40%) females with a mean age of 25.09 years with a range of 8-44 years. The major clinical features included tenderness in the right iliac fossa, vomiting, palpable mass in the right iliac fossa, anorexia and diarrhea. Tachycardia and fever were other vital signs observed. 85% of the patients had a leukocytosis of more than 10000/cm, while a neutrophilia of >75% was present in 90% of cases. Ultrasound of the abdomen detected a mass in the right iliac fossa in 30 (60%) patients, while the remaining 20 (40%) cases were identified at operation. A simple mass composed of an inflamed appendix. Omentum was found in 30 cases, pelvic abscess 5 cases, intussusception in one case, fish bone in one case, vermicularis in one case, gangrene of the omentum in one case and Fecolith in 4 cases. The pattern of operative findings and operative problems differed significantly in both groups, as shown in Table 1.

Table 1. Operative findings in both groups
Immediate appendectomy needed lengthening of the incision to overcome the difficulty in dissection due to adhesions in 9 (18%) patients. The pattern of postoperative complications in both groups is shown in Table 2.

Table 2. Post-operative findings in both groups.
The total hospital stay in group A patients included only 3-5 day hospital admission compared to group B patients who were admitted 7-10. In group B, total patients treated conventionally, 35 (70%) were successfully operated on after 4-8 weeks. Seven patients refused interval appendectomy, and in 13 patients, we had to stop the conservative treatment and resort to operation because of the deteriorating condition of the patients. Five of these patients had perforated appendices, which led to spreading peritonitis. Eleven patients were lost to follow-up and never returned for interval appendectomy. Patients on conservative management remained hospitalized for 7-10 days during their first admission and for another 4-8 days after interval appendectomy.

Table 3. Comparison of HbA1C with another parameter.
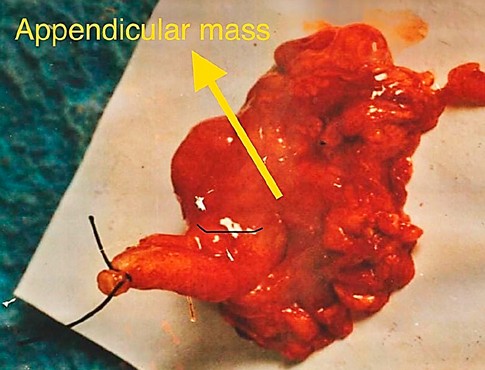
Figure 1. Appendicitis mass.
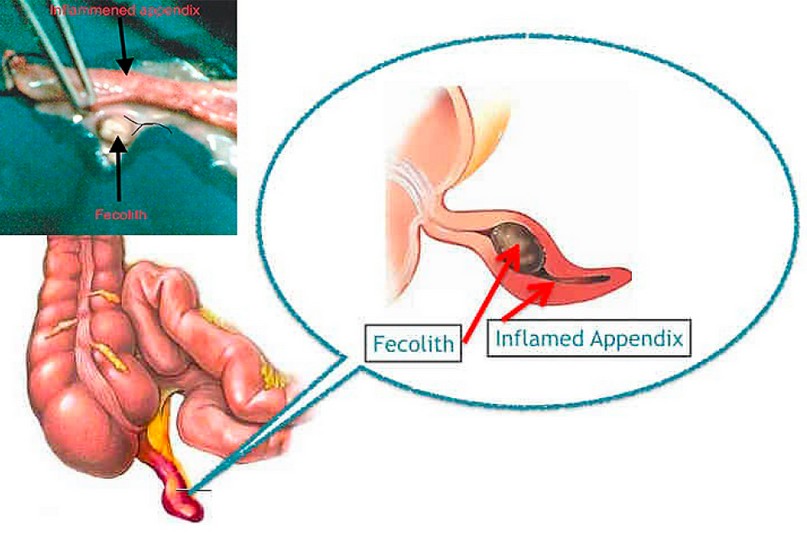
Figure 2. Appendix obstructed by Fecolith.
DISCUSSION
The treatment of appendicular mass is taking a turn from the traditional approach of initial conservative treatment followed by interval appendectomy to immediate appendectomy14, 15. However, these changes are not widely accepted, and many surgeons continue to adopt the same traditional conservative approach16. Because it significantly shortens the overall hospital stay and prevents the need for a second readmission, early surgical intervention has long been recognized as a successful and alternative conservative approach17. This leads to reducing the total expenses substantially. The conventional treatment comprises hospitalization, intravenous fluids, antibiotics, analgesics and strict monitoring of the vitals and general state of the patient. In 0-20% of the cases, it proves unsuccessful, and patients need emergency operation due to spreading infection, which is comparatively more difficult18, 19. In addition, patients may suffer a recurrence of appendicitis after being discharged from the hospital20, 21. Many patients effuse readmission for operation once their acute problem is solved, which seems to be a significant advantage of the initial conservative approach. Another disadvantage of conservative management is the chance of misdiagnoses like intussusception and carcinoma caecum, fish bone, Fecolith and vermicularis, but in early surgery; we can deal with it and early return to work. Our study highlights the feasibility and effectiveness of early appendectomy in appendicular mass, and the results are consistent with several similar studies22, 23. Early appendectomy is a more appropriate and effective way of managing Appendicular mass. Early appendectomy has several benefits, including a fully curative procedure, shorter hospital stays, minimum morbidity, and patient compliance. Due to an overall improvement in anesthesia, supportive care, and antibiotics, the old opinion that surgery is complex in states when the inflamed appendix is deeply embedded in the mass, and the intestinal loops are friable is more relevant now. The operative problems such as localization of appendix, adhesiolysis and bleeding are more pronounced and troublesome with interval appendectomy as shown findings of this study. Wound infection, however, remains a common postoperative complication of early appendectomy in appendicular mass, but the rate of wound infection is not so high as to preclude this early operative approach. The benefits of early appendectomy overweigh the results of interval appendectomy as evident from our results and also supported by many other studies referred to in comparison to our findings.
CONCLUSIONS
Early appendectomy on appendiceal mass is a safe and effective alternative to conventional conservative treatment followed by interval appendectomy. It reduces mortality, morbidity and hospital readmission for surgery, mainly when caused by fishbone-induced appendicitis, vermicularis, omentum gangrene, fecoliths and intussusception. This reduced this problem and patients' hospital stay and early return to work, making it safer and effectively better than conservation treatment.
Funding: This research received no external funding.
REFERENCES
1. Arshad, M., et al., Early appendicectomy in appendicular mass–a Liaquat University Hospital experience. J Ayub Med Coll Abbottabad, 2008. 20(1): p. 70-2.
2. Khurana, J.S. and K.K. Unni, Pathological diagnosis of common tumors of bone and cartilage, in Handbook of Histology Methods for Bone and Cartilage. 2003, Springer. p. 447-494.
3. Shipsey, M.R. and B. O'Donnell, Conservative management of appendix mass in children. Annals of The Royal College of Surgeons of England, 1985. 67(1): p. 23.
4. Nitecki, S., A. Assalia, and M. Schein, Contemporary management of the appendiceal mass. Journal of British Surgery, 1993. 80(1): p. 18-20.
5. Senapathi, P., D. Bhattacharya, and B. Ammori, Early laparoscopic appendectomy for appendicular mass. Surgical Endoscopy And Other Interventional Techniques, 2002. 16(12): p. 1783-1785.
6. Russel, R., N. William, and C. Bulstaode, Diabetic gangrene in Russel RCG. William NS, Bulstraode CJK Bailey and love's short practice of surgery, 24th ed, London: Arnold, UK, 2004: p. 219-20.
7. Vargas, H.I., A. Averbook, and M.J. Stamos, Appendiceal mass: conservative therapy followed by interval laparoscopic appendectomy. The American Surgeon, 1994. 60(10): p. 753-758.
8. Ein, S.H. and B. Shandling, Is interval appendectomy necessary after rupture of an appendiceal mass? Journal of pediatric surgery, 1996. 31(6): p. 849-850.
9. Eriksson, S. and J. Styrud, Interval appendicectomy: a retrospective study. The European journal of surgery, 1998. 164(10): p. 771-774.
10. Tingstedt, B., et al., management of appendiceal masses. The European journal of surgery, 2002. 168(11): p. 579-582.
11. Choudry, Z., A. Syed, and P. Mishra, Early exploration or appendicular mass. Pak. J. Surg, 1996. 12(2): p. 64-66.
12. Vakili, C., Operative treatment of appendix mass. The American Journal of Surgery, 1976. 131(3): p. 312-314.
13. Al-Samarrai, A.Y.I., Surgery for appendicular mass. Saudi Journal of Gastroenterology, 1995. 1(1): p. 43.
14. Patel, B.J. and K.H. Patel, A comparative study of appendicular lump management. International Surgery Journal, 2016. 2(2): p. 235-238.
15. Price, M.R., et al., Recurrent appendicitis after initial conservative management of appendiceal abscess. Journal of pediatric surgery, 1996. 31(2): p. 291-294.
16. Erdoğan, D., et al., Comparison of two methods for the management of appendicular mass in children. Pediatric surgery international, 2005. 21(2): p. 81-83.
17. Jordan, J., P. Kovalcik, and C. Schwab, Appendicitis with a palpable mass. Annals of surgery, 1981. 193(2): p. 227.
18. Foran, B., T.V. Berne, and L. Rosoff, Management of the appendiceal mass. Archives of Surgery, 1978. 113(10): p. 1144-1145.
19. Janik, J.S., et al., Nonsurgical management of appendiceal mass in late presenting children. Journal of Pediatric Surgery, 1980. 15(4): p. 574-576.
20. Bagi, P. and S. Dueholm, Nonoperative management of the ultrasonically evaluated appendiceal mass. Surgery, 1987. 101(5): p. 602-605.
21. Oliak, D., et al., Nonoperative management of perforated appendicitis without periappendiceal mass. The American Journal of Surgery, 2000. 179(3): p. 177-181.
22. De, U. and S. Ghosh, Acute appendicectomy for appendicular mass: a study of 87 patients. The Ceylon medical journal, 2002. 47(4): p. 117-118.
23. Samuel, M., G. Hosie, and K. Holmes, Prospective evaluation of nonsurgical versus surgical management of appendiceal mass. Journal of pediatric surgery, 2002. 37(6): p. 882-886.
Received: September 22, 2022 / Accepted: October 18, 2022 / Published:15 November 2022
Citation: Al-Obaidi J H. Early appendectomy in appendicular mass. Revis Bionatura 2022;7(4) 67. http://dx.doi.org/10.21931/RB/2022.07.04.67