2023.08.04.83
Files > Volume 8 > Vol 8 no 4 2023

Ashwaq Audah
Department of Community Health, Techniques,
Al-Furat Al-Awsat Technical University, Technical Institute, Samawa, Iraq
*Correspondence: Email:
[email protected]
Available
from: Available from. http://dx.doi.org/10.21931/RB/2023.08.04.83
ABSTRACT
Foundation: Kidney
disappointment is an ailment in which the kidneys no longer function. (1) It is
isolated into intense kidney disappointment (cases that proliferate) and
persistent kidney disappointment (those that are long haul). Indications might
incorporate leg expansion, feeling tired, heaving, loss of craving, or
disarray. Complexities of intense infection might incorporate uremia, high
blood potassium, or volume over-burden. Difficulties of ongoing illness might
incorporate coronary illness, hypertension, or sickliness. Creatinine is a
breakdown result of creatine phosphate in muscle and is generally delivered at
a genuinely consistent rate by the body (contingent upon bulk). Point:
This study expects to research the connection between catalase compound,
creatinine, and urea level with the advancement of kidney disappointment.
Techniques: Plasma of Catalase, creatinine, and Urea were not entirely settled
in 46 patients with kidney disappointment and 21 solid subjects as control
bunch utilizing the colorimetric technique. All outcomes were genuinely
examined. Results: A profoundly huge increment was found in the serum level of
creatinine and urea in patients with Kidney disappointment contrasted with
control (P < 0.05). Compared with the control, serum levels of catalase
compound were diminished in the patient gathering (P < 0.05). End: The
consequences of the current review give proof that the family background of
kidney infection, diabetes mellitus, hypertension, coronary illness, and
long-haul uncontrolled hypertension has an unmistakable connection with kidney
disappointment hazard. Undeniable degrees of creatinine and urea were
introduced in patients with Kidney disappointment.
Keywords: Catalase enzyme, Creatinine, Urea, Kidney failure Diseases.
INTRODUCTION
Kidney dissatisfaction, called end-stage kidney sickness, is
an affliction wherein the kidneys work under 15% of run-of-the-mill levels1.
Kidney frustration is named either extraordinary kidney dissatisfaction, which
develops rapidly and may resolve, and constant kidney disillusionment, which
develops progressively and can frequently be irreversible2.
Appearances could consolidate leg amplification, tiredness, regurgitation, loss
of craving, and confusion3. Complexities of extreme and continuous
disillusionment join uremia, high blood potassium, and volume overload4.
Complexities of continuous frustration similarly fuse coronary sickness,
hypertension, and anemia5. A creatinine test is the extent of how
well kidneys are playing out their control of filtering waste from your blood,
and creatinine is an engineered compound left over from energy-conveying
processes in muscles. Vital kidneys channel creatinine out of the blood.
Creatinine exits the body as a side-effect of pee. An assessment of creatinine
in your blood or pee offers hints to help experts conclude how well the kidneys
are working6.
Creatinine
is an engineered side-effect of creatine, an amino destructive made by the
liver and set aside in the liver. Creatinine is the eventual outcome of common
muscle metabolism7. The substance enters your dissemination
framework after it is isolated. Kidneys dispose of it from blood. The
creatinine then leaves the body through pee. Run-of-the-mill levels vary, as
demonstrated by your body size and muscle mass8. For example, a
standard reach for men is between 0.6 and 1.2 mg/dl, and a regular reach for
women is 0.5 and 1.1 mg/dl. Uremia means kidney disillusionment. Whenever the
kidneys cannot channel waste to form, it can enter the bloodstream9
A
considerable number of individuals with uremia will require dialysis. Dialysis
uses a machine to go comparably a "fake kidney" that channels the
blood10. Some may require a kidney move, which could thwart further
kidney issues by overriding a sickly kidney with a strong one. People routinely
need to hold on for various years for a kidney and may require dialysis while
they stop. Many indications are called uremic neuropathy or nerve pain on
account of kidney disillusionment. Neuropathy can cause shuddering, deadness,
or electrical sensations in the body, particularly the hands and feet. These
signs will regularly fall apart over an extended period and do not vanish with
rest or further sustenance: nausea, regurgitating, and loss of hankering.
Certain people could get in shape by these issues—changes in blood tests. The
critical sign of uremia frequently is the presence of urea in the blood during
routine blood testing12.
Catalase
is a tetrameric peroxidase protein that changes H2O2 to water and nuclear
oxygen. Essentially, using H+ advocates, catalase works with diminishing normal
hydroperoxide (ROOH+AH2→H2O+ROH+A). H2O213 oversees the quality enunciation of
catalase. In animals, H2O2 is detoxified by catalase and GPX. Catalase shields
the cells from H2O2, and 14 plays a critical role in the disease
anticipation specialist monitoring structure and change to oxidant stress15.
In vertebrates, catalase is considered to be pervasively in the liver. A couple
of factors affect the rate at which a substance works. In this review, we
estimated that degrees of level creatinine, urea and catalase chemicals are
markers of Kidney disappointment expansion in Kidney disappointment patients.
To test our theory, we looked at pattern creatinine, urea and catalase catalyst
levels in kidney and non-kidney disappointment patients.
MATERIALS AND METHODS
Serum
creatinine, urea and catalase compound levels were estimated in 21
solid people—also 46 patients with Kidney disappointment. The mean time of
control (47.93±3.05) and the patient gathering (46.73±3.54) were arbitrarily
chosen from patients with Kidney disappointment from walk to October 2021. Data
regarding the clinical history of each Subject was obtained, including age,
infections endured, and term of disease with their day-by-day diet and
occupation.
Techniques
All
gatherings were exposed to exhaustive clinical history, assessment and explicit
Kidney disappointment examination. Venous blood tests (5 ml) were gathered from
the patient and control gatherings. The serum was isolated by centrifugation
(Gallen Germany) at 3000 RPM for 10 min and put away in covered plastic
cylinders at -20 °C until examination. The serum's creatinine, urea and
catalase catalyst levels were estimated using the Spectrophotometric strategy
at at532 nm 548 nm by utilizing Shimadzu U.V-Noticeable recorder
spectrophotometer model U.V-160. The last focus was communicated in pg/ml.
Factual investigation
Information
is communicated as mean ± SEM. A statistical investigation was done utilizing a
plan, measurable bundle for sociology (SPSS), and the stark contrasts between
the control and the patients were not entirely settled by utilizing an
understudy's t-test. The likelihood of (P<0.05) is considered critical all
through.
RESULTS
Clinical
characteristics about patients’ age and so forth were summarized in (Table 1).
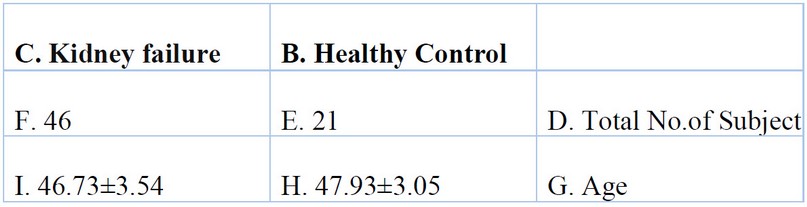
Table 1. General Characteristics of Healthy Controls and Kidney Failure
Patients (Cases).
Serum
Creatinine and urea levels were found to be significantly higher in Kidney failure patients compared to control (p< 0.05, Fig.1 and Fig.2).
Catalase enzyme was significantly decreased in the serum of Kidney failure patients compared to control (P <0.05, Fig.3).
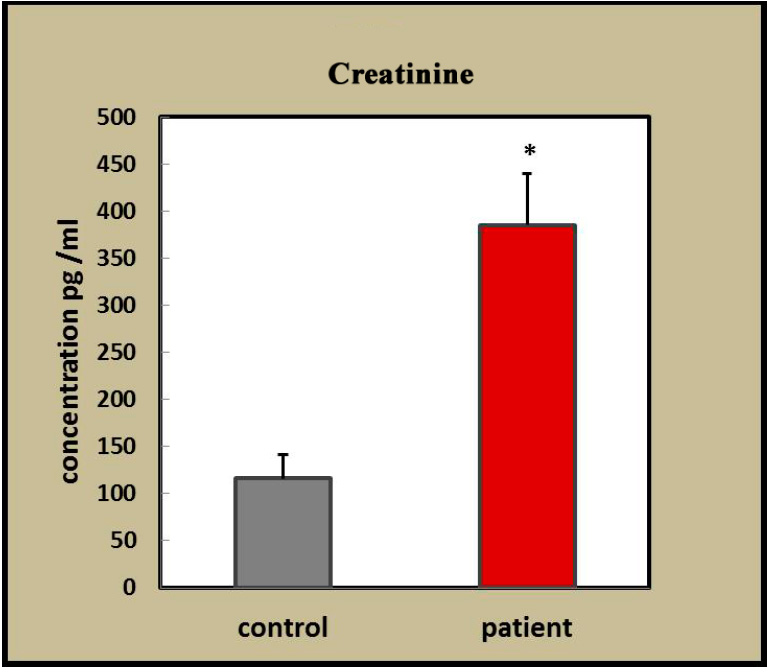
Figure 1. Creatinine levels in healthy patients at (p<0.05).
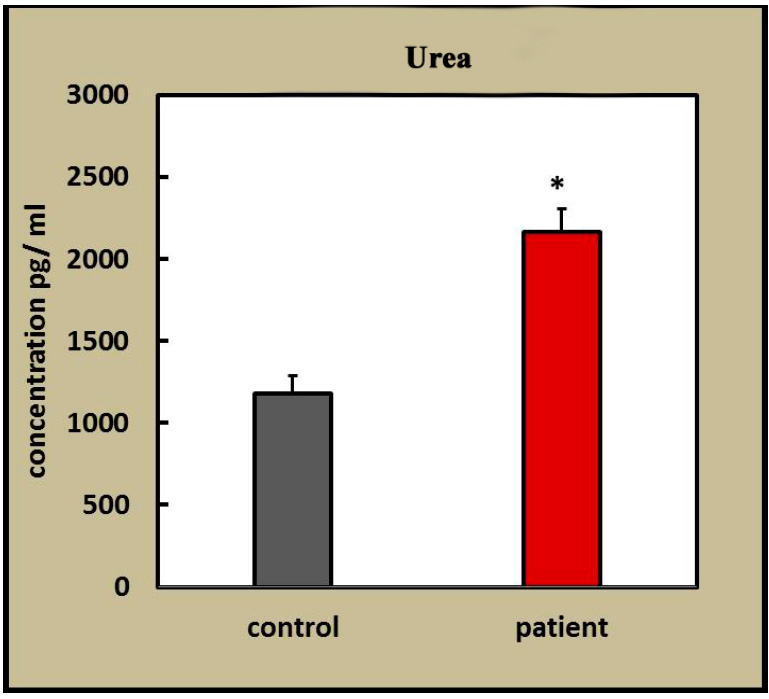
Figure 2. Urea levels in healthy and patient (p<0.05).
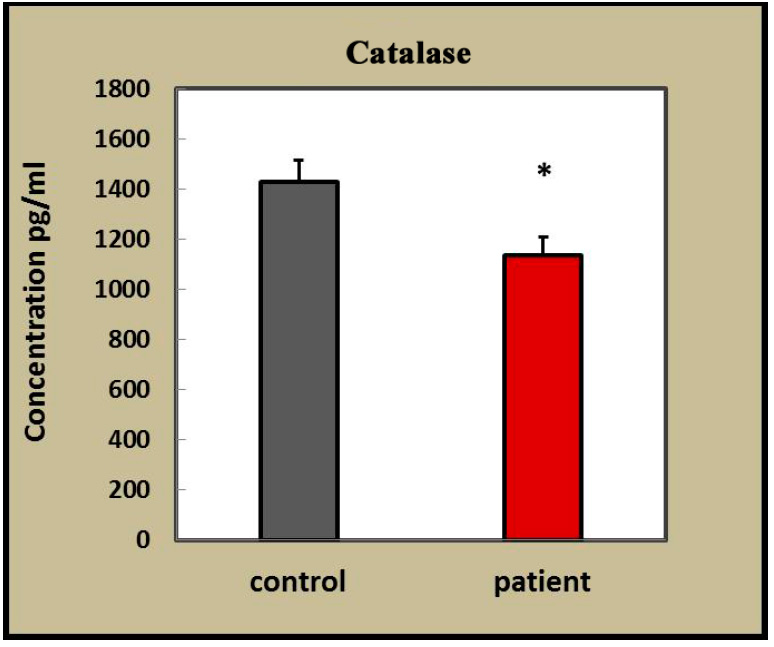
Figure 3. Catalase enzyme levels in healthy patients (p<0.05).
DISCUSSION
Kidney disappointment is a non-kidding, long-term condition
that influences the kidneys and causes an expanding and progressive loss of
kidney work and renal disappointment in the last stage21. In
persistent renal disappointment, kidney work drops to under 25% of the ordinary
level. In this jumble over the years, the kidneys progressively lose their
capacity to channel squanders from the blood and dispose of them in the pee.
Therefore, the gathering of liquids in the body and poisons, for example, Urea
and Creatinine in the blood, happens because of the powerlessness of the
kidneys to channel the blood going through them, so its worth expansions in
This is the thing seen in the exploration, which prompts not many indications
from the get-go. Nosigns might only show up once most kidney work has been
lost. Constant renal disappointment (CRF) is related to oxidative pressure that
adds to the advancement of various short- and long-haul complexities, including
hypertension, frailty, arteriosclerotic cardiovascular sickness, neurological
issues, hemostatic anomalies, and disabled resistance. The presence of
oxidative pressure in CRF is proven by an excess of side-effects of
collaboration of responsive oxygen species (ROS) with and decline Catalase
compound levels have been accounted for in Kidney disappointment 5.
Our outcomes showed a decline in Catalase chemical level in Kidney
disappointment when contrasted with controls, concurring with past studies22.
While the presence of oxidative pressure in CRF is grounded,
its hidden systems have, as of late, been unfurled. Oxidative pressure can
happen either because of expanded ROS age, discouraged cell reinforcement
framework or both. The standard cell reinforcement framework comprises a
progression of cancer prevention agent catalysts and various endogenous and
dietary cancer prevention agents that respond with and inactivate ROS. The
essential ROS created in the high-impact life forms is superoxide, an exceptionally
responsive and cytotoxic specialist 14. The most proficient catalyst
is catalase, as every chemical can perform roughly 800,000 synergist occasions
each second. The primary capacity of catalase is to safeguard cells from
hydrogen peroxide (H2O2) particles by changing them to oxygen and water. In
this review, we showed that serum levels of creatinine urea are fundamentally
expanded in Kidney disappointment when contrasted with solid subjects. In the
current review, creatinine urea level has been reliably exhibited to be raised
in patients with Kidney disappointment. Declining: Declining the viability of
catalase chemicals in kidney disappointment prompts oxidative and tissue harm
because of the increment in free extremists and the absence of cell
reinforcements.
CONCLUSIONS
In conclusion, kidney failure is a serious
condition that leads to a progressive loss of kidney function and the
accumulation of toxins in the body. Oxidative stress plays a role in the
development of complications associated with kidney failure, and the
effectiveness of catalase enzymes is reduced, leading to tissue damage.
REFERENCES
1.
Paul, N.K. Man, N. Moatti, D. Raichvarg. Membrane
phospholipid peroxidation in renal insufficiency and chronic hemodialysis,
Nephrology, 1991; 12 , pp. 4-7.
2.T. Miyata, K. Kurokawa, C. Van
Ypersele De Strihou. Advanced glycation and
lipoxidation end products: role of reactive carbonyl compounds generated during
carbohydrate and lipid metabolism. J. Am. Soc. Nephrol.
2000, 11 pp. 1744-1752.
3.
N.D. Vaziri, Z. Ni, F. Oveisi, K. Liang.
Enhanced nitric oxide inactivation and protein nitration by reactive oxygen
species in chronic renal insufficiency. Hypertension,2002 39 (2002),
pp. 135-141.
4.
J. Himmelfarb, E. McMonagle. Albumin is the major plasma protein
target of oxidant stress in uremia. Kidney Int. 2001, 60 ,
pp. 358-363.
5.
N.D. Vaziri, F. Oveisi, Y. Ding (1998). Role of
increased oxygen free radical activity in the pathogenesis of uremic
hypertension. Kidney Int., 1998, 53 ; pp. 1748-1754.
6.
H. Muhammed, S., Y. Mohamed, R. Investigation And Molecular Identification Of
Cucumber Damping-Off Fungi Under Greenhouse Condition. Anbar Journal Of
Agricultural Sciences, 2023; 21(1): 19-31. doi: 10.32649/ajas.2023.179712.
7.
R.K. Sindhu, J.R. Koo, C.K. Roberts, N.D. Vaziri.
Dysregulation of hepatic superoxide dismutase, catalase and glutathione
peroxidase in diabetes: response to insulin and antioxidant therapies. Clin.
Exp. Hypertens. 2004, 26 , pp. 43-53.
8.
N.D. Vaziri, Z. Ni, F. Oveisi, K. Liang, R. Pandian.
Enhanced nitric oxide inactivation and protein nitration by reactive oxygen
species in renal insufficiency. Hypertension, 2002; 136 ,
pp. 135-141.
9.
Al-Atijawi, S. H. .; Almusawy, R. S. . The Effect Of Adding Different Rates Of
Mushroom Powder To The Wheat Flour On The Nutritional Value Of Proteins,
Sensory And Physical Properties Of Local Bread. JLSAR 2021, 2, 46–53.
10.
O. Sommerburg, T. Grune, J.H. Ehrich, W.G. Siems.
Adaptation of glutathione peroxidase activity to oxidative stress occurs in
children but not in adult patients with end-stage renal failure undergoing
hemodialysis. Clin. Nephrol., 2002 58 (Suppl. 1) ,
pp. S31-S36.
11.
J. Mimic-Oka, T. Simic, L. Djukanovic, Z. Reljic, Z. Davicevic
(1999). Alteration in plasma antioxidant capacity in various degrees of chronic
renal failure. Clin. Nephrol.,1999. 51 , pp. 233-241.
12.
G. Sener, K. Paskaloglu, H. Toklu, C. Kapucu, G. Ayanoglu-Dulger, A. Kacmaz, A. Sakarcan.
Melatonin ameliorates chronic renal failure-induced oxidative organ damage in
rats J. Pineal Res. 2004, 36 , pp. 232-241.
13.
C. Van den Branden, B. Ceyssens, D. De
Craemer, P. De Bleser, K. Hellemans, A. Greerts, D. Verbeelen.
Antioxidant enzyme gene expression in rats with remnant kidney induced chronic
renal failure. Exp. Nephrol. 2000, 8 , pp. 91-96.
14.
T. Zima, S. Stipek, J. Crkovska, K. Nemecek, J. Platenik, V. Bartova, V. Tesar.
Antioxidant enzymes—superoxide dismutase and glutathione peroxidase—in
haemodialyzed patients. Blood Purif. 1996, 14, pp. 257-261.
15.
N.D. Vaziri, X.Q. Wang, F. Oveisi, B. Rad.
Induction of oxidative stress by glutathione depletion causes severe
hypertension in normal rats. Hypertension, 2000; 36 ,
pp. 142-146.
16.
C. Van den Branden, B. Ceyssens, D. De
Craemer, M. Pauwels, K. Vanden Houte, P. De
Bleser, K. Hellemans, A. Geerts, D. Verbeelen.
Renal antioxidant enzymes and fibrosis-related markers in the rat adriamycin
model. Nephron, 2000; 86 , pp. 167-175.
17.
J.S. Koenig, M. Fischer, E. Bulant, B. Tiran, I. Elmadfa, W. Druml.
Antioxidant status in patients on chronic hemodialysis therapy: impact of
parenteral selenium supplementation. Wien. Klin. Wochenschr. 1997, 109 ,
pp. 13-19.
18.
C.K. Roberts, N.D. Vaziri, R.K. Sindhu, R.J. Barnard.
A high-fat, refined-carbohydrate diet affects renal NO synthase protein
expression and salt sensitivity. J. Appl. Physiol. 2003, 94 ,
pp. 941-946.
19.
Ibraheem M W, Muhaimeed A R, Mohammed Th. T. Leg cuts from Awaasi lambs fed a
diet with varying levels of Rhus coriaria L., Physical dissection and chemical
composition. Revis Bionatura 2022;7(4) 4.
http://dx.doi.org/10.21931/RB/2022.07.04.4.
20.
R.A. Beswick, A.M. Dorrance, R. Leite, R.C. Webb.
NADH/NADPH oxidase and enhanced superoxide production in the mineralocorticoid
hypertensive rat. Hypertension, 2001; 38 , pp. 1107-1111.
21.
K. Trznadel, L. Pawlicki, J. Kedziora, M. Luciak, J. Blaszczyk, A. Buczynski.
Superoxide anion generation, erythrocytes superoxide dismutase activity, and
lipid peroxidation during hemoperfusion and hemodialysis in chronic uremic
patients. Free Radic. Biol. Med. 1989, 6 , pp. 393-397.
22.
M. Inal, G. Kanbak, S. Sen, F. Akyuz, E. Sunal.
Antioxidant status and lipid peroxidation in hemodialysis patients undergoing
erythropoietin and erythropoietin-vitamin E combined therapy. Free Radic. Res.
1999, 31 , pp. 211-216.
Received: 26 September 2023 / Accepted: 15 April 2023 / Published: 15
December 2023
Citation: Audah, A. The
antioxidant status of Kidney failure patients. Revis Bionatura
2023;8 (4) 83. http://dx.doi.org/10.21931/RB/2023.08.04.83
Publisher’s Note: Bionatura stays neutral with regard to
jurisdictional claims in published maps and institutional affiliations.
Copyright: © 2022 by the
authors. Submitted for possible open access publication under the terms and
conditions of the Creative Commons Attribution (CC BY) license
(https://creativecommons.org/licenses/by/4.0/).